Pectus excavatum, or sunken chest, is the most common congenital chest wall abnormality in children. Although some may think of the abnormality as purely a cosmetic problem, the limited chest cavity space can displace the heart as well as limit lung capacity, says Dr. Mustafa Kabeer, a pediatric surgeon at CHOC.
Fifteen percent of patients can experience arrhythmia (an abnormal heart rhythm) or mitral valve regurgitation, wherein the heart valves allow blood to leak back into the heart, as a result of the inward compression from the sternum.
Surgery to expand the chest wall can eliminate many symptoms. The pediatric surgeons at CHOC perform the Nuss procedure to repair pectus excavatum.
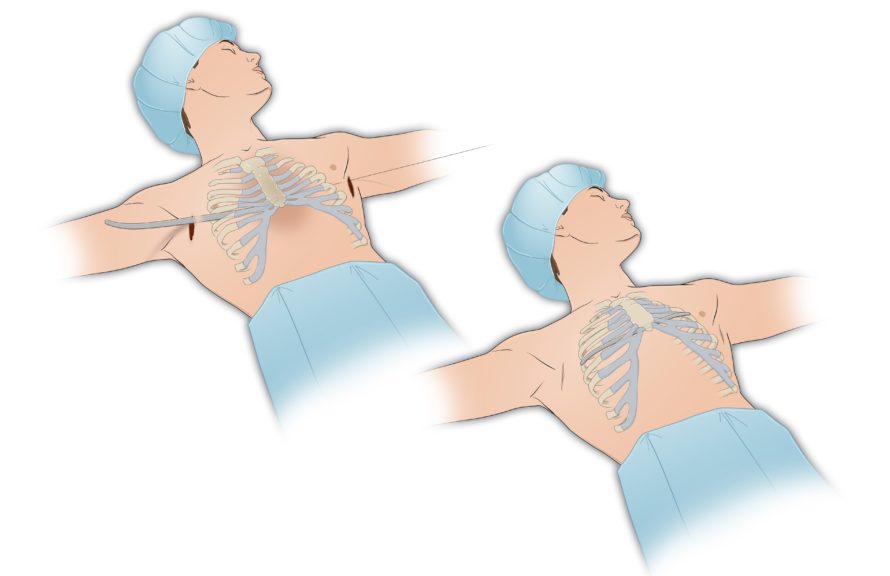
The Nuss procedure is a newer, minimally invasive procedure that dramatically reduces the appearance of incisions and the time spent in the operating room. A small incision is made on either side of the chest, and a small camera is inserted for observation as the surgeon passes a thin, curved metal bar through the chest cavity below the sternum. When the bar is flipped, the sunken chest is instantaneously repaired. The bar remains in place for two years, and is periodically monitored by a pediatric surgeon.
A historical approach to these surgeries involved a large incision across the chest, and up to six hours in the operating room as the chest wall was taken apart and then reconstructed, known as the Ravitch procedure. There can also be significantly greater blood loss with the Ravitch procedure, and virtually none with the Nuss procedure.
The pectus excavatum team at CHOC is comprised of experts in pediatric pulmonology, cardiology and surgery. The multidisciplinary team performs various tests to examine heart and lung function, before and after surgery. By using the latest techniques in minimally invasive surgery, along with recent improvements in pain management, patients are able to return home and get back to their daily activities sooner than ever before.
Although the cause is unknown, 40 percent of patients report a family history of pectus excavatum, and 40 percent of cases occur in tandem with scoliosis, says Kabeer.
Parents may notice an indentation in their child’s chest wall either when they are first born, or closer to puberty, when changes in the chest wall can become more pronounced.
“When pectus excavatum presents itself closer to puberty, it may be difficult for parents to notice, since teens or pre-teens are more clothed than they were as babies, so their parents might not see the change in their chest wall right away,” says Kabeer.
Warning signs tend to be subtle, but if your child experiences frequent shortness of breath, difficulty breathing during exercise, chest pain or light- headedness, or otherwise is not able to keep up with their peers, consult your child’s primary care physician, who may refer you to a pediatric surgeon or pectus excavatum specialist.