Medical insights from Dr. Donald Shaul, a board-certified pediatric surgeon at Rady Children’s Hospital Orange County (Rady Children’s)
Helping caretakers make sense of anorectal malformation and imperforate anus
Learning that your baby has an anorectal malformation or an imperforate anus can feel scary and confusing. Many families have never heard these terms before birth. This guide explains what they mean in clear language, why they happen, and how doctors treat them.
First, what is a “congenital condition”?
A congenital condition is a health difference a baby is born with. It develops early in pregnancy while the baby’s organs are forming. Nothing a parent does during pregnancy causes an anorectal malformation, it is simply the way the baby’s body developed.
What are anorectal malformations?
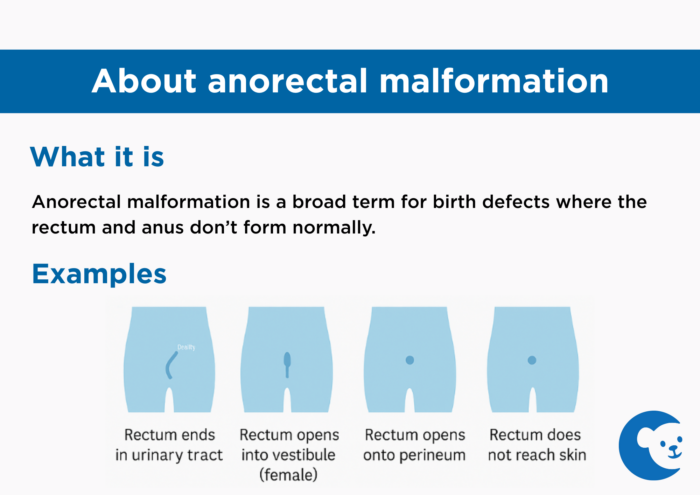
Anorectal malformation (ARM) is a broad term for conditions where the rectum and anus don’t form in the typical way before birth. The rectum is supposed to grow downward and connect to the skin in the middle of the anal sphincter muscles. These muscles help control bowel movements.
In an ARM, this connection doesn’t form correctly. The rectum may:
- Stop before reaching the skin
- Connect to the urinary tract (more common in boys)
- Open into the vaginal area, called the vestibule (in girls)
- Open onto the perineum — the skin between the genitals and where the anus should be
All of these are considered anorectal malformations.
What is an imperforate anus?
An imperforate anus is a common type of anorectal malformation. It means the anal opening is missing, blocked, or in the wrong place. Because of this, a baby cannot pass stool normally.
Think of imperforate anus as one specific diagnosis within the larger ARM family.
What happens right after birth?
Many babies with an ARM or imperforate anus are taken to the neonatal intensive care unit (NICU) shortly after birth so they can be checked carefully and gently.
Doctors will:
- Examine the baby to understand the type of malformation
- Check for other conditions that can occur with ARM
- Decide whether the baby needs a colostomy
A colostomy is a temporary opening on the belly that allows stool to exit into a small bag. If needed, it is usually done within the first 48 hours of life. Some babies do not need a colostomy right away and can go home while doctors plan the best approach.

How doctors plan surgery
Babies with these conditions are usually cared for in a specialized colorectal clinic. This clinic includes surgeons, nurses and other experts who guide families through every step, from learning about the condition to planning surgery and follow‑up care.
The main goal of surgery is always the same: Move the rectum into the center of the anal sphincter muscles so the baby can pass stool normally.
The approach depends on the exact type of ARM.
Examples of surgical approaches
- Rectoperineal fistula (simpler type):
The rectum is close to the right spot and not attached to other organs. Doctors make a small opening and move it into place.
- Rectum connected to the bladder (more complex, usually in boys):
The rectum must be gently separated from the urinary system before being moved.
- Rectovestibular fistula (common in girls):
Often doesn’t require a colostomy at birth. Doctors may gently widen the small opening so stool can pass. Later, they move the rectum to the center of the sphincter muscles.
- Cloaca (most complex):
The rectum, urinary tract, and reproductive tract share one opening. These cases require very specialized surgical care.
Recovery after surgery
Most babies stay in the hospital for two to three days after surgery. Newborns may need a little longer. When they go home, families get clear instructions on how to care for the surgical site.
Doctors carefully monitor the new anal opening to make sure it heals and stays open. Sometimes families are asked to perform dilations, which means gently placing a small tool into the anus to prevent narrowing as it heals. This usually lasts a few months.
If the baby had a colostomy earlier, it is usually closed once healing is complete
Choosing the right surgical team matters
Repairing an imperforate anus or any anorectal malformation is a delicate surgery. Families should look for a team with:
- Many years of experience
- A well‑established colorectal program
- A history of treating a high number of ARM cases
- Coordinated care from newborn assessment through recovery
You only get one chance at the first repair, and the best outcomes come from teams who do this often and do it well.
Moving forward
Although the diagnosis can feel overwhelming, most babies with anorectal malformations do very well after surgery. With expert care and ongoing support, children can grow, thrive, and enjoy active childhoods.
You are not alone and our experienced teams are ready to guide your family every step of the way.
Related stories:
Get more expert health advice delivered to your inbox monthly by subscribing to the KidsHealth newsletter here.
Learn more about the CHOC’s Colorectal and Urogenital Center
The CHOC Colorectal and Urogenital Center specializes in providing expert diagnosis and second opinions for colorectal disorders, as well as developing personalized treatment plans using advanced diagnostics and the latest research-based treatment options.